Understanding Nerve Anatomy in Dentistry
Dental care relies on knowing where nerves run in the jaws and face. Most feeling in the teeth, gums, and lips comes from branches of the trigeminal nerve. These branches travel through bone canals and soft tissues, sometimes very close to teeth roots. Knowing their paths helps plan safer treatment.
Picture this: before a tooth is removed, the surgeon reviews your scan to see every nearby nerve. The main nerves dentists consider include:
- Inferior alveolar nerve, inside the mandibular canal, giving feeling to lower teeth.
- Mental nerve, exiting the mental foramen to supply the lower lip and chin.
- Lingual nerve, in the soft tissue on the tongue side of lower molars.
- Long buccal nerve, supplying cheek-side gums near lower molars.
- Posterior superior alveolar nerves, along the maxillary sinus wall to upper molars.
- Infraorbital nerve, giving sensation to upper lip, cheek, and anterior teeth region.
- Greater palatine and nasopalatine nerves, serving the palate.
Small changes in nerve location matter. The inferior alveolar nerve can run very near the roots of lower wisdom teeth, and the lingual nerve may lie close to the inner bony plate behind them. Careful imaging and gentle soft tissue handling lower risk during wisdom tooth removal. The mental foramen position varies too, so incisions or implants in the premolar area require precise mapping.
In the upper jaw, nerve branches often track along the sinus walls, and root tips may approach the sinus floor. The infraorbital canal is nearby when treating canines or placing anterior implants. Palatal nerves run in fixed grooves, so flap design respects those routes. Cone beam CT helps visualize these spaces in three dimensions, which supports nerve injury prevention oral surgery planning. This is equally important for precise placement of full arch implants.
Understanding nerve anatomy guides safer procedures and clearer informed consent. Better maps make gentler dentistry.
Importance of Nerve Injury Prevention
Preventing nerve injury in oral surgery protects the feeling and function of your lips, tongue, and teeth. When nerves stay healthy, speech, chewing, and smile control feel normal, and recovery is smoother. Thoughtful planning and technique lower the chance of numbness, tingling, or altered taste after procedures. This is central to effective nerve injury prevention oral surgery.
Even small injuries can cause temporary or lasting changes, so prevention starts before the first incision. Picture this: before placing a lower implant, a scan shows the nerve canal closer than expected. Pre‑surgical imaging, including cone‑beam CT, helps map nerve position, gauge distances to roots, and tailor the plan. Studies show CBCT can reveal close relationships between molar roots and the mandibular canal, guiding safer choices in approach and instrumentation [1]. This same mapping supports safer implant placement, including careful planning for snap‑in implant dentures.
In the operating room, prevention continues with gentle soft‑tissue handling, protective retraction, and conservative bone removal. Surgeons may adjust the design of flaps, select shorter implants, or change angulation to keep a safe buffer from nerve canals. For high‑risk lower wisdom teeth, staged or partial removal can be considered to avoid traction on nearby nerves. Careful drilling with steady speed and irrigation limits heat and pressure on deeper structures. Outside of surgery, precise working lengths and apical control matter during root canal treatment in the lower jaw, where over‑instrumentation or overfill could irritate nearby neural tissues. Each of these steps stacks small safety margins into meaningful protection.
For patients, this means fewer surprises, clearer consent, and a more comfortable recovery. Asking how your dentist or surgeon plans imaging, nerve mapping, and intraoperative safeguards can help you understand your specific risk. Good prevention supports healthy sensation, confident chewing, and long‑term comfort. Thoughtful planning protects feeling and function.
Risks Associated with Nerve Injury
Nerve injury during oral surgery can change how areas of the mouth feel and work. You might notice numbness, tingling, burning pain, altered taste, or trouble moving the tongue normally. These changes can affect speech, chewing, and daily comfort. Many issues improve over time, but some can last.
Picture this: after a lower wisdom tooth removal, the lower lip feels numb for days. Nerves can be irritated by stretching, pressure, heat from drilling, or direct cutting. Swelling or bleeding within tight spaces can also compress a nerve. In the lower jaw, injuries may involve the inferior alveolar or lingual nerves, which influence lip and tongue sensation. In the upper jaw, branches near the sinus and front teeth can be affected, sometimes changing feeling in the cheek or upper lip.
The impact ranges from mild tingling to painful hypersensitivity that makes light touch feel sharp. Biting or burning soft tissues is easier when areas are numb, so careful self‑care is important until feeling returns. Early signs of recovery often include pins‑and‑needles, then gradual return of normal sensation over weeks to months. Clinical studies of high‑risk lower wisdom tooth surgery track inferior alveolar nerve neurosensory outcomes, and adjuncts such as platelet‑rich plasma have been evaluated to support recovery [2]. If symptoms worsen or do not change after several weeks, timely evaluation helps guide next steps.
Understanding these risks helps you prepare and ask focused questions before treatment. Your care team can explain your specific nerve proximity, what symptoms to watch for, and how to protect numb tissues during healing. This knowledge also supports better nerve injury prevention oral surgery planning and informed consent. Next, we outline how clinicians assess sensation and monitor progress after procedures.
Preoperative Planning Strategies
Preoperative planning sets the course for a safer, smoother surgery. It means studying your anatomy, reviewing your health history, and choosing techniques that protect nearby nerves. The goal is to foresee challenges, reduce surprises, and build safety margins before any incision. Before surgery, the team meets to review your scan and choose the safest path.
Planning starts with precise imaging and mapping. Cone beam CT or targeted radiographs help locate nerve canals, foramina, and soft tissue paths. The surgeon measures key distances, selects a safe approach, and designs the access so instruments work away from nerves. Surgical guides or navigation may be used for accurate implant positioning. If a third molar or implant site sits very close to a nerve, the plan can change to a staged approach, altered angulation, or a different tooth sectioning strategy. These steps form the backbone of nerve injury prevention oral surgery.
Next, soft tissue plans aim to protect nerves you cannot see on X‑rays. Flap design anticipates where the lingual and mental nerves run, and retraction plans keep pressure off those areas. The drilling sequence is chosen to limit heat and vibration, with steady speed and irrigation. For high‑risk sites, shorter or narrower implants are considered to keep a safe buffer. In some cases, coronectomy or partial root removal reduces traction on deep structures while still addressing the problem tooth.
Medical and patient factors are addressed before the day of surgery. The team reviews medications, bleeding risks, and prior surgeries that might change nerve location or tissue response. They also plan anesthesia, communication, and positioning so you remain comfortable and still. If anxiety is high, your provider can discuss preparing for oral sedation as part of a calm, well‑paced visit.
For patients, good planning means clearer consent, fewer surprises, and a recovery focused on healing instead of troubleshooting. Ask how imaging, access, and instrument choices will protect nearby nerves in your case. Thoughtful preparation leads to safer care. Good plans protect sensation and comfort.
Techniques for Minimizing Risks
Clinicians reduce nerve risks by mapping anatomy, controlling instruments, and protecting soft tissues at every step. The core methods include precise imaging, guided access, careful retraction, and cool, conservative drilling. Used together, these techniques lower the chance of altered feeling and support effective nerve injury prevention oral surgery.
Picture this: during lower implant placement, a surgical guide keeps the drill clear of the canal. Planning starts with measuring safe distances on scans, then using static guides or real‑time navigation to keep angulation and depth within a planned envelope. Pilot drills with depth stops, frequent length checks, and gentle tapping rather than prying protect nearby canals and foramina. When landmarks are unclear, a quick intraoperative radiograph or navigation checkpoint helps confirm the path before proceeding.
Access design matters. Flaps are planned so instruments work away from the lingual nerve, and retractors rest on stable bone with minimal pressure. The mental foramen is identified on the scan, and incisions or releasing cuts are shifted to avoid it. For high‑risk third molars, sectioning the tooth into smaller parts or choosing a coronectomy can reduce traction on deep structures. These small choices stack safety margins without adding much time.
Thermal and mechanical control protect nerves you cannot see. Drilling with sharp burs, steady speed, light pressure, and copious irrigation limits heat. Short, intermittent cuts allow cooling and tactile feedback. Near vital structures, piezoelectric or fine hand instruments can reduce unintended soft‑tissue contact. If local anesthesia is used, slow, low‑pressure injection with aspiration helps avoid intraneural injury, and clinicians pause if a sudden “electric” sensation is reported.
Patient comfort supports precision. Good anesthesia, clear communication, bite blocks, and gentle jaw support reduce movement, which keeps instruments on plan. For longer or complex procedures, discussing deep sedation options may help maintain stillness and a calm experience. If you want to know when these services are available, check our current hours. Safer technique begins with careful planning and steady, well‑cooled instrumentation.
The Role of Imaging in Surgery
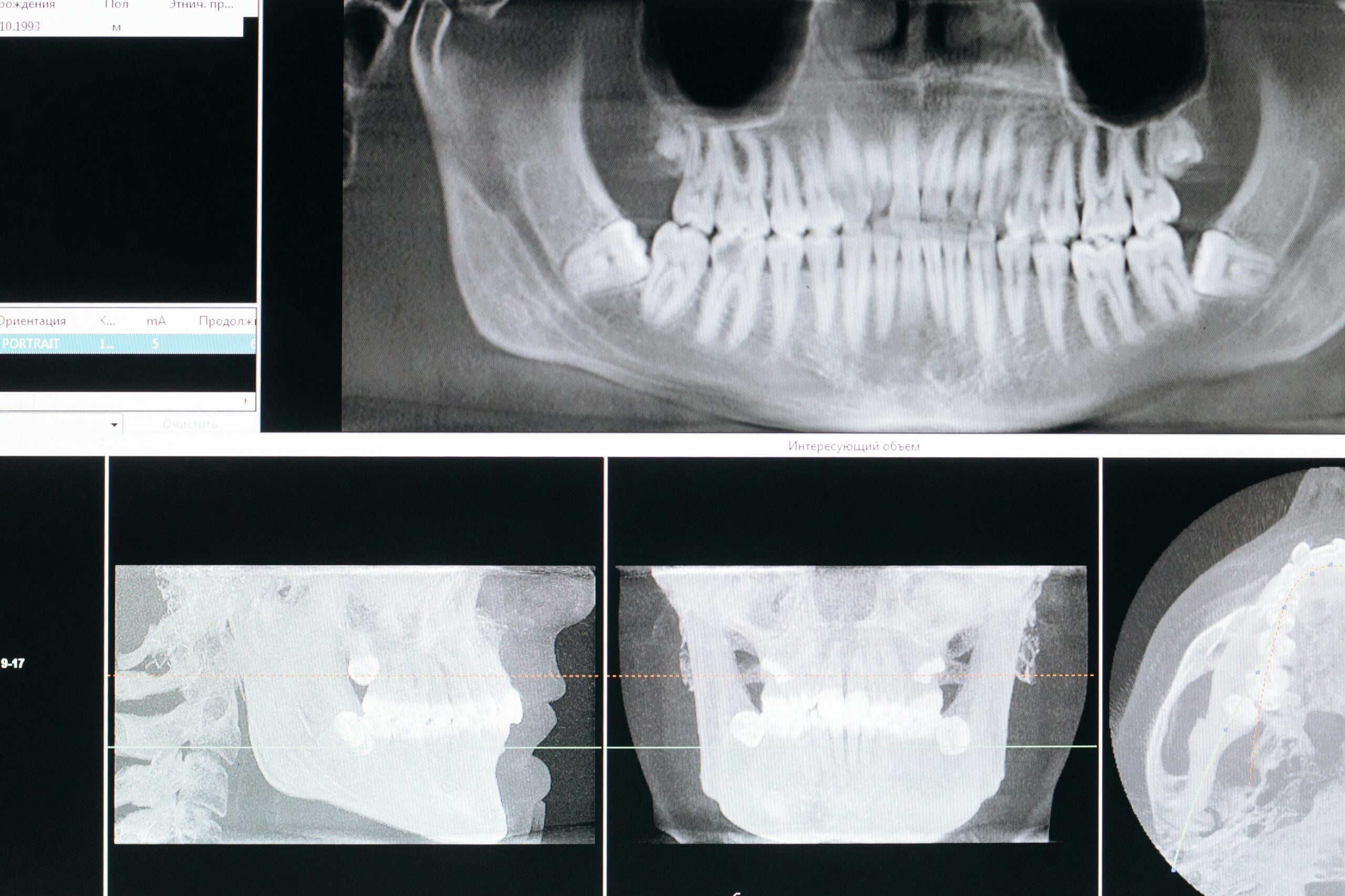
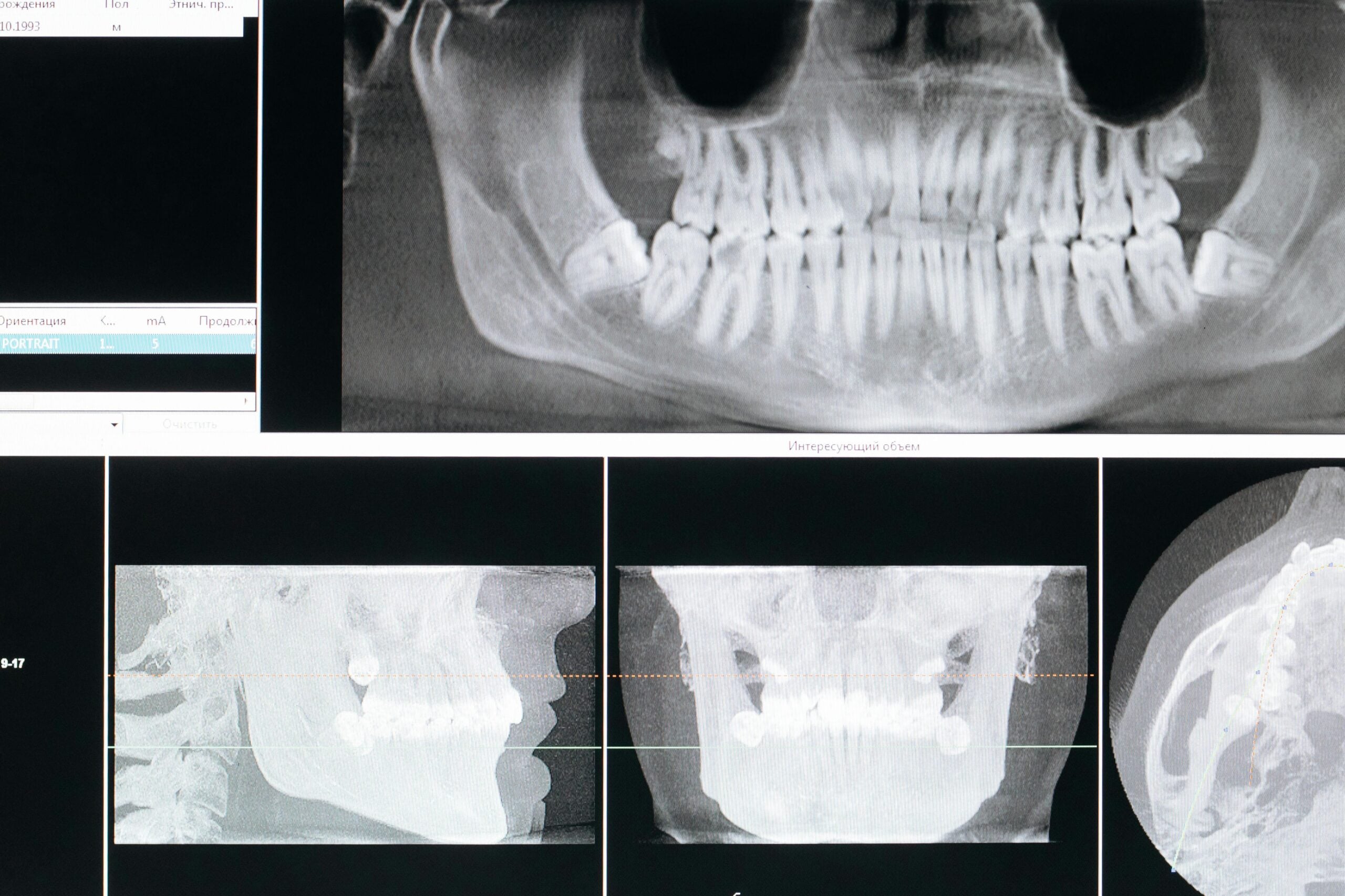
Imaging shows where teeth, bone, and nearby nerves actually are, so surgery can be planned with confidence. It helps the surgeon choose the safest path, anticipate challenges, and protect sensation. Before removing an impacted canine, a 3D scan can reveal the exact course of a nearby nerve. Clear pictures lead to clearer, safer steps.
Different images answer different questions. A panoramic radiograph gives a broad map of jaws and sinuses, useful for screening root positions and canal paths. Periapical films add fine detail around a specific tooth. Cone beam CT (CBCT) builds a three‑dimensional view, letting the team trace the mandibular canal, locate the mental foramen, and see the lingual concavity or sinus floor in true 3D. After a screening image raises a question, CBCT clarifies depth and proximity so the plan can be adjusted before instruments touch bone.
CBCT settings are tailored to the task. A limited field of view targets only the area of interest, while appropriate voxel size balances detail with image noise. Positioning and exposure settings help reduce metal streaks from fillings or brackets, which keeps nerve outlines visible. With accurate data, surgical guides or navigation can be designed to control angulation and depth, keeping drills within a planned envelope. If landmarks seem unclear once surgery begins, a quick intraoperative radiograph can confirm orientation before proceeding.
Imaging also shapes how access is designed. Knowing the mental foramen location allows small shifts in incision or release cuts to avoid traction on that bundle. Tracing the inferior alveolar canal informs implant length and trajectory, and viewing root curvature guides safe sectioning of difficult third molars. Seeing the sinus floor or nasal floor in 3D helps set conservative limits for osteotomy depth. These choices stack safety margins that support nerve injury prevention oral surgery.
For patients, better imaging means fewer surprises, clearer consent, and a plan that fits your anatomy. It can shorten procedures by preventing detours, and it provides a baseline to compare if sensation changes after treatment. Good pictures make safer decisions. Thoughtful imaging protects feeling and function.
Intraoperative Considerations and Care
Intraoperative care focuses on protecting nerves while the procedure is underway. The team controls access, retraction, and drilling so instruments stay a safe distance from nerve pathways. Real‑time checks, steady technique, and clear communication help prevent sudden pressure, heat, or traction on delicate structures. These steps keep sensation as normal as possible after surgery.
Picture this: during a lower molar extraction, the surgeon pauses when you feel a quick jolt. That pause matters. Gentle, stable retraction on bone, not soft tissue, reduces stretch on the lingual nerve. Flap edges are placed to avoid the mental foramen, and release cuts are shifted when needed. When anatomy looks tighter than expected, the approach is adjusted before deeper steps are taken.
Instrument control is the backbone of safety. Depth is confirmed often, using pilot paths, physical stops, and frequent irrigation to keep bone cool. Short, intermittent cutting allows tactile feedback and limits heat buildup. Near vital structures, fine hand instruments or piezoelectric tips can help avoid accidental soft‑tissue contact. If a patient reports an “electric” sensation during local anesthesia or drilling, the clinician repositions and reassesses before continuing. Slow injection with aspiration lowers the chance of intraneural needle placement.
Preventing compression is just as important as avoiding cuts. Careful hemostasis limits pressure inside tight bony spaces, and bone edges are smoothed so tissues rest without pinch points. When a third molar or implant site sits very close to a canal, the team may stage treatment or choose partial tooth removal to reduce traction. Before closure, the field is rinsed, visual landmarks are rechecked, and sutures are placed to support a calm, low‑tension heal. This measured approach supports nerve injury prevention oral surgery without adding unnecessary steps.
For patients, these choices mean fewer surprises and a smoother recovery. Asking how your team manages retraction, depth control, and cooling can clarify your personal risk and plan. Thoughtful technique during surgery protects sensation and comfort.
Postoperative Monitoring and Support
Postoperative monitoring and support focus on checking nerve function, guiding comfort, and acting early if changes appear. Your care team tracks sensation, taste, and movement, then compares findings over time. Clear instructions help you protect numb areas while healing. If something does not follow the expected course, the plan is adjusted quickly.
Day two after surgery, your lip still feels numb. Early on, lingering local anesthetic can blur what you feel, so the first check confirms that normal numbness is fading and that no new tingling, burning, or weakness is emerging. Short follow‑ups look for steady improvement, not perfection. If symptoms worsen or expand, your dentist documents the change and reassesses sooner.
In the clinic, neurosensory testing is simple and repeatable. Light touch, gentle pinprick, and temperature checks map what you feel and what you do not. Two‑point discrimination can show whether detail is returning, and for tongue symptoms, taste on each side is compared. The edges of any altered area are drawn on a chart or photo so progress is easy to see at later visits. Using the same tests each time makes trends clear and decisions more confident.
Home care supports this process. Chew on the opposite side until feeling improves, and take care with hot foods so you do not burn numb tissues. Use a mirror to check for accidental lip or tongue bites, and report any injuries or drooling. Keep notes on changes, such as new pins‑and‑needles or shrinking numb zones, and share them at follow‑ups. If sharp, electric pains start, or if there is no improvement over the expected early window, timely evaluation and possible referral are considered.
When monitoring is structured and communication stays open, small gains are noticed and problems are addressed early. This steady approach supports nerve injury prevention oral surgery by catching changes before they become lasting. Ask your team what to expect and when to check in. Early checks guide safe healing.
Patient Education and Communication
Patient education and communication mean explaining risks, choices, and what to expect in clear, simple terms. When you understand where nearby nerves are and how surgery may affect them, you can give informed consent and help protect those areas. Good two‑way communication lowers anxiety and supports safer care. It is a vital part of nerve injury prevention oral surgery.
Picture this: before surgery, your dentist shows your scan and traces the nerve canal on the screen. You learn what normal numbness from local anesthesia feels like, how long it usually lasts, and which warning signs need a call. The team also explains how to protect numb tissues, such as avoiding hot drinks until feeling returns and watching for accidental lip or tongue bites. Before any anesthesia, they check and document current lip and tongue sensation so changes after surgery are easier to spot.
To keep the plan clear, the team uses plain language, short summaries, and simple diagrams that mark high‑risk zones. The “teach‑back” approach helps confirm understanding, by asking you to repeat the key steps for protection and when to seek help. If you prefer another language or have hearing or vision needs, interpreters or adapted materials are offered so nothing important is missed. If anxiety makes it hard to focus, the provider can slow the pace, pause for questions, and review options for comfort so you can stay still and relaxed.
Communication continues during surgery. You agree on a stop signal, and if you feel a sudden “electric” jolt, the team pauses and reassesses. Before you leave, you receive written instructions with simple symptom checklists, expected timelines, and who to contact if concerns arise. Early follow‑up is scheduled to review sensation, answer questions, and adjust the plan if needed. Accurate notes from these visits guide next steps and keep everyone aligned.
Clear education and open dialogue help you take an active role in protecting sensation and healing well. Next, structured monitoring turns these conversations into careful checks and timely support. Good communication makes safer dentistry.
Addressing Nerve Injury Concerns
Addressing nerve injury concerns starts with clear information, careful checks, and a plan that fits your situation. We explain what is normal after anesthesia or surgery, what warning signs to watch for, and how sensation usually returns. If you notice numbness, tingling, or burning, we map what you feel, compare both sides, and set follow‑up times. The goal is to answer questions early and act quickly when needed.
Picture this: after a dental injection, your tongue still feels numb the next morning. First, we confirm the local anesthetic has fully worn off and note exactly which areas feel different. Simple neurosensory tests check light touch, pinprick, and temperature, then two‑point discrimination tracks detail over time. We record a baseline, explain expected timelines for improvement, and give you clear instructions for protecting numb tissues.
Next, we look for clues that guide the plan. A brief “electric” jolt during injection or drilling can mean the needle or instrument brushed a nerve. Swelling or tight spaces can also compress a nerve, so we assess the surgical site and bite for pressure points. If findings suggest close proximity to a canal or foramen, targeted imaging may help confirm safe distances and rule out mechanical causes we can correct. Most minor nerve irritations improve over days to weeks, with pins‑and‑needles often marking early recovery. If symptoms are severe, spreading, or unchanged after an expected window, we discuss additional options, including timely referral to a clinician experienced in nerve assessment.
Comfort and self‑care matter throughout recovery. Chew on the opposite side, test food temperatures carefully, and use a mirror to avoid lip or tongue bites. Keep notes on changes, including new tingling or shrinking numb areas, and bring them to follow‑ups. For bothersome sensations, your provider may consider medicines that target nerve pain, short‑term topical care, or supportive therapies, matched to your exam and progress. Regular check‑ins keep the plan current and reduce uncertainty.
When concerns are addressed early and documented well, small gains are easier to see and problems are caught sooner. Clear answers and timely checks are part of nerve injury prevention oral surgery. Most patients heal well with informed guidance.
Long-Term Outcomes and Prognosis
Most nerve changes after oral surgery improve over time, though the pace varies. Many patients notice better feeling within weeks to months, and some continue to gain sensation for up to a year. A few people have lasting numbness or altered feeling, but stable function is still common. Prognosis depends on how close the procedure was to a nerve and the type of injury.
Three months after lower molar surgery, tingling replaces earlier numbness. This pattern often suggests healing. Mild stretch or pressure injuries usually recover as swelling settles and nerve fibers resume signaling. Deeper injuries, where some fibers are disrupted, heal more slowly because regrowth takes time. A complete cut is rare, but has the most guarded outlook and may need specialist input.
What you feel can hint at the path ahead. Early pins and needles, shrinking numb areas, and better two‑point detail point toward recovery. Persistent, dense numbness that does not change for several months, or burning pain that disrupts daily life, is more concerning. Age, smoking, systemic health, and the length of the affected nerve segment also influence results. Careful mapping with simple tests at each visit makes trends clear and guides next steps.
Timelines are gradual. Many improvements appear in the first 6 to 8 weeks, then continue in smaller steps. Gains often plateau by 6 to 12 months, and that plateau usually reflects the long‑term outcome. Even when sensation is not perfect, most patients adapt well with protection habits and, when appropriate, desensitization exercises or medicines selected by their provider. If progress stalls, targeted imaging and a focused exam can look for causes that are still correctable.
Prevention shapes prognosis. Thoughtful planning, precise imaging, and steady technique reduce the chance of lasting change, which is the aim of nerve injury prevention oral surgery. If you have lingering symptoms, structured follow‑up and open communication help set expectations and support safe healing. Most patients regain comfortable, useful sensation over time.
Frequently Asked Questions
Here are quick answers to common questions people have about Preventing Nerve Injury in Oral Surgery in Glendale, AZ.
- How can nerve injuries during oral surgery be prevented?
Preventing nerve injuries starts with careful planning and imaging, like using cone beam CT scans to map nerves near teeth and bones. Surgeons choose safe paths and adjust techniques to avoid nerves. This includes gentle handling, precise drilling, and protecting soft tissues. Thoughtful preparation helps shield nerves during oral surgery, reducing risks of numbness or tingling. Regular check-ups allow timely adjustment if issues arise, ensuring safe outcomes.
- What is the role of imaging in preventing nerve injuries during surgery?
Imaging, such as cone beam CT, provides a 3D view of the teeth, nerves, and bones, crucial for planning safe surgeries. It helps locate nerve paths and measure safe distances, allowing surgeons to avoid them. Imaging aids in designing surgical guides and planning techniques, thereby reducing the risk of nerve injuries. It ensures safety margins and tailored surgical strategies for optimal patient outcomes.
- What are the risks associated with nerve injuries in oral surgery?
Nerve injuries during oral surgery can lead to numbness, tingling, or pain in affected areas. These symptoms might impact daily activities like speaking and chewing. While many recover over time, some effects may be lasting. Managing risks requires understanding nerve locations and using surgical techniques that minimize potential damage. Regular monitoring and communication with healthcare providers help address any concerns promptly.
- How does preoperative planning help in minimizing nerve injuries?
Preoperative planning involves reviewing imaging to map nerve paths, studying health history, and selecting safe surgical techniques. This planning helps anticipate challenges and reduce surprises, promoting safer procedures. By designing surgeries that avoid nerve areas, surgeons create safety buffers that lower the risk of nerve damages, assisting in smoother surgery and recovery.
- What are the long-term outcomes for nerve injuries after oral surgery?
Most nerve injuries gradually improve, with some recovering sensation over weeks to months. Minor injuries typically heal as swelling subsides, while more severe cases may require longer recovery times. Prognosis depends on factors like the location of the nerve and any underlying health conditions. Long-term outcomes are often positive with careful monitoring and treatment adjustments.
References
- [1] Assessment of mandibular canal proximity to molar root apices in a Turkish subpopulation: A cone-beam computed tomography study. (2026) — PubMed:41758202 / DOI: 10.17219/dmp/163216
- [2] Effect of intraoperative platelet-rich plasma on inferior alveolar nerve neurosensory outcomes after high-risk mandibular third molar extraction. (2026) — PubMed:42001493 / DOI: 10.4317/medoral.28126