The following case was an interesting and fairly difficult root canal procedure from a week ago. I normally see maybe one or two of these cases each week, but it has been almost a month since the last one. My patient was a 67-year old male with no remarkable health conditions. He was experiencing vague pain symptoms on the right side which ultimately made diagnosis difficult. Because I want to share my work more consistently, I was sure to document the case to share with you here.
Root Canal Diagnosis
This case was especially difficult to diagnose. The patient was experiencing vague pain symptoms on the right side for several months that was provoked by drinking cold beverages. He was convinced it was coming from a top tooth but wasn’t sure. The patient had a crown done less than one year earlier by a different dentist on his upper-right molar.
Imaging
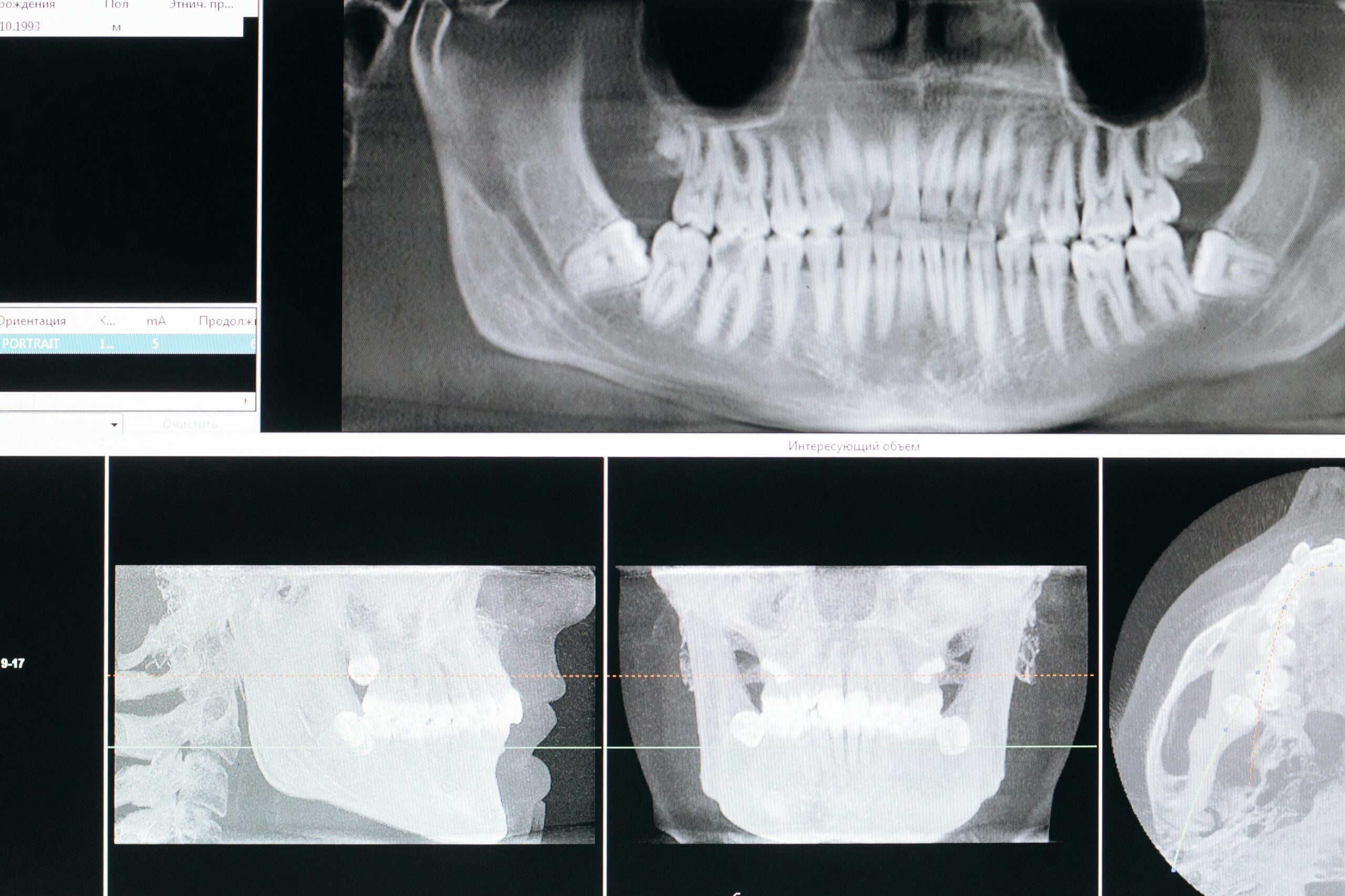
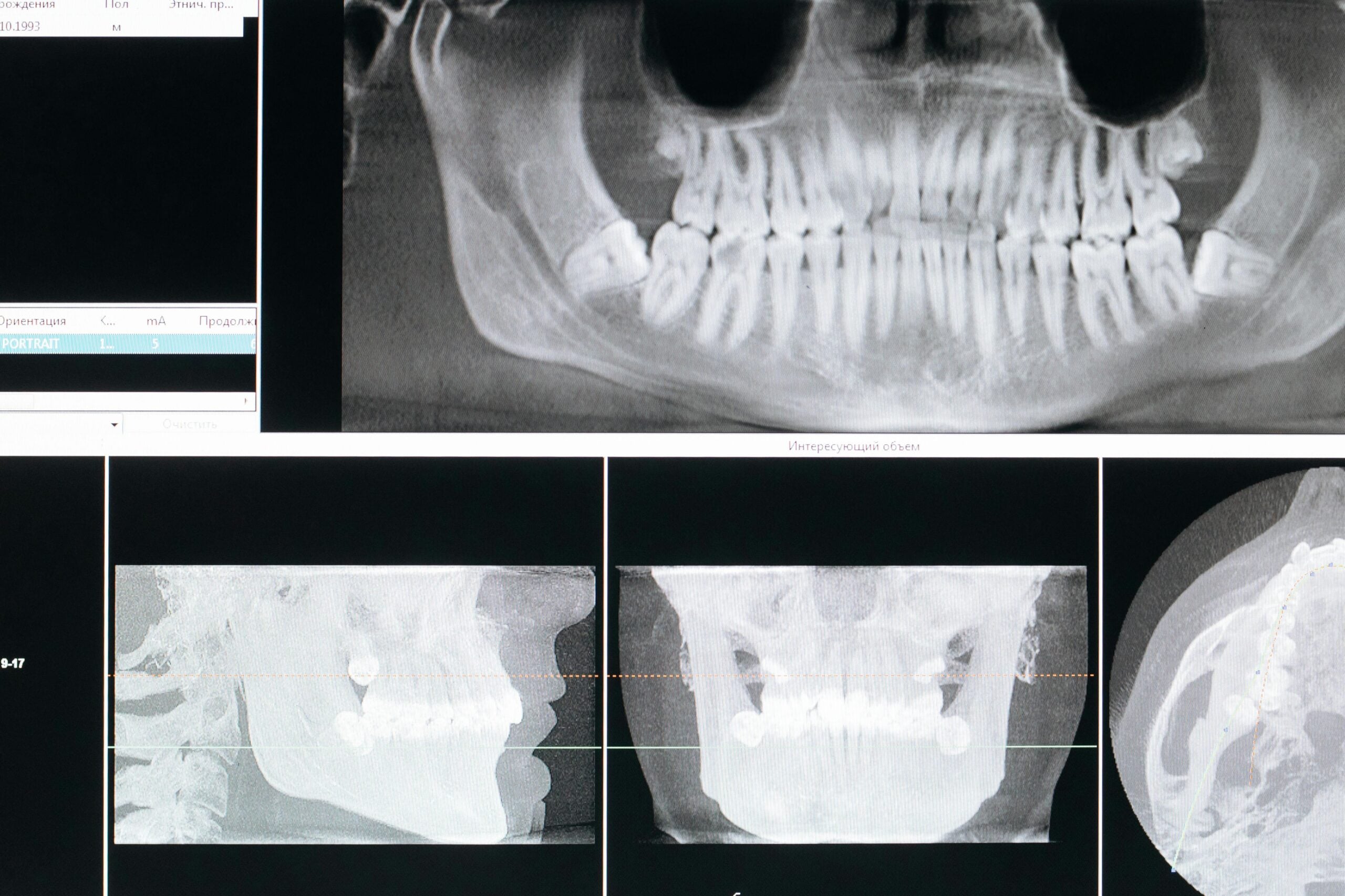
The x-ray we took seemed to show early signs of infection, but I still wanted to be sure we had the right tooth before jumping in. In addition to the original x-ray, we also acquired a Cone Beam CT Scan (CBCT) of the tooth. Still, I wasn’t 100% sure we had the right tooth as the appearance of PDL expansion we saw on both images is also commonly seen in healthy teeth.


Percussion
When I am trying to identify the problem tooth, I will usually tap on it to see how the patient responds. Often just tapping the offending tooth elicits the pain response so common to infected teeth in need of a root canal. This time, tapping didn’t cause pain on any the teeth on his right side, not even the one I suspected.
Cold Testing
Whether tapping indicates a painful tooth or not, I always follow-up with thermal testing. Basically, I put something cold against the tooth and see how the patient responds. My patient nearly jumped out of the chair when I touched a molar on the lower-right side, but not the tooth I anticipated would need the root canal. This response contradicted the patient’s complaint of pain from an upper tooth and the x-ray that seemed to show a small abscess on the upper-right molar. However, sometimes referred pain from a bottom tooth can make it seem like the pain is coming from a top tooth.

I decided to investigate the lower-right molar fully and either confirm or rule it out. Our initial x-rays showed nothing remarkable with that tooth. So, we of the lower-right molar and still saw nothing significant. I wanted to be absolutely sure we treated the correct tooth, so I had the patient drink ice water so I could see his normal pain response. Then, I numbed the patient’s lower jaw and had him drink cold water again. He experienced the same painful stimulus as he had before. So, I numbed the upper-right molar I had suspected earlier and had him drink again. This time, there was no pain. I was confident that we had found the offending tooth.
Planning the Root Canal


Now that I am confident I’ve got the right tooth, I set about planning the case. When it comes to root canals, I don’t like surprises, and patient’s want to spend as little time in the chair as possible. One of the best ways to eliminate surprises and reduce chair times is to use CBCT technology to map the morphology of the patient’s root canal system. If there are extra canals, we will know about them before we ever cut into the tooth. This way, I don’t waste time looking for canals that may or may not be there.
Morphology
Generally, about half of maxillary second molars will have just three canals in three separate roots. This is the most common configuration, and the one most dentists look for when performing a root canal on an upper second molar. However, a large number have a fourth canal which shares a root with another canal. Our patient has four canals, as you can see in the CBCT image shown above.
Health Factors
Our patient is a 67-year old male with no remarkable medical history. His age means we can expect the canals of this tooth to be sclerotic. As people age, the canals inside of their teeth tend to become smaller. This complicates root canal treatments because smaller canals are harder to find and even harder to clean out properly.
Other Factors
Lastly, we are treating a tooth that has a crown. Normally, when we put a hole in the top of a tooth for a root canal, we are following important landmarks that are visible on the surface of the tooth. When the tooth has a crown on it, those landmarks don’t usually reflect how the tooth looked before. Also, crowns can block light, making it even harder to see inside the tooth.
Root Canal Treatment

After numbing the patient, the first thing I do when performing a root canal procedure is place a dental dam. The dental dam is a device that prevents contaminants from entering the tooth after we have opened it up. Also, the dental dam protects the patient from instruments, debris, or chemicals entering their mouth.
When I’m confident the dental dam is in position, and the patient signals that they are ready, I put a hole in the tooth. We call this “accessing” the tooth. Ideally, we keep the hole as small as possible to preserve the structural integrity of the tooth.
Once I access the tooth, I immediately begin to disinfect the inside before searching for canals. When I have removed all of the soft pulpal tissues from inside the tooth, I then begin the hunt for all of the canals.

Next, we find the canals and clean them all out thoroughly. Part of the cleaning process involves shaping the canals to allow for a sealer to be placed. In our patient’s case, his canals were fairly straight forward but one of the canals (MB2) took extra time and effort to complete. Upper molars often feature difficult anatomy and additional canals, this is why they take longer, it is also the reason many dentists refer them to specialists.
Finishing the Root Canal
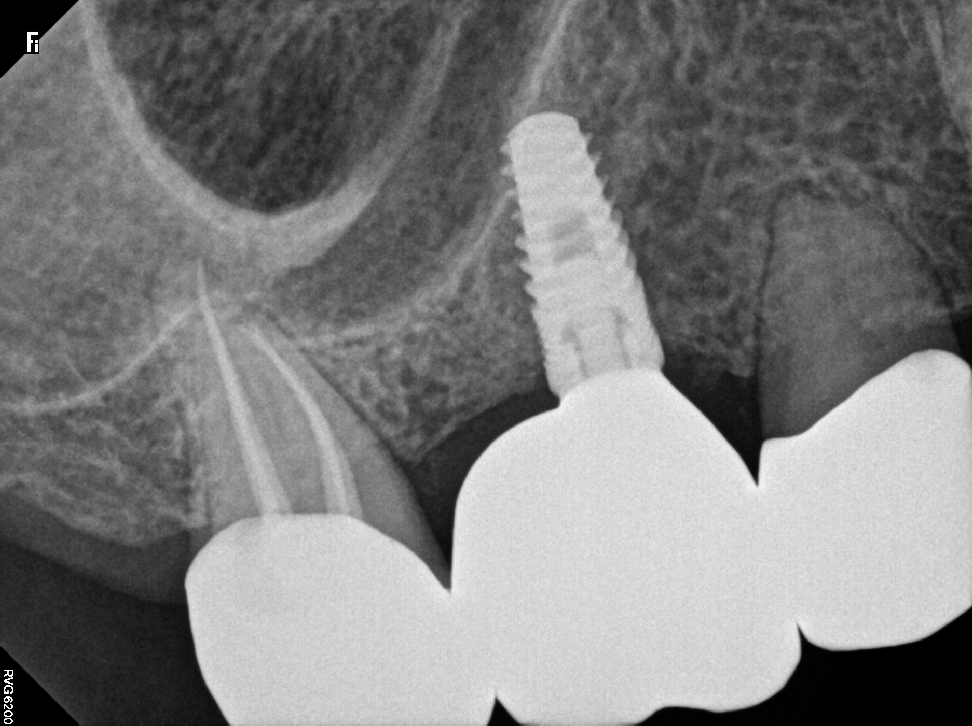
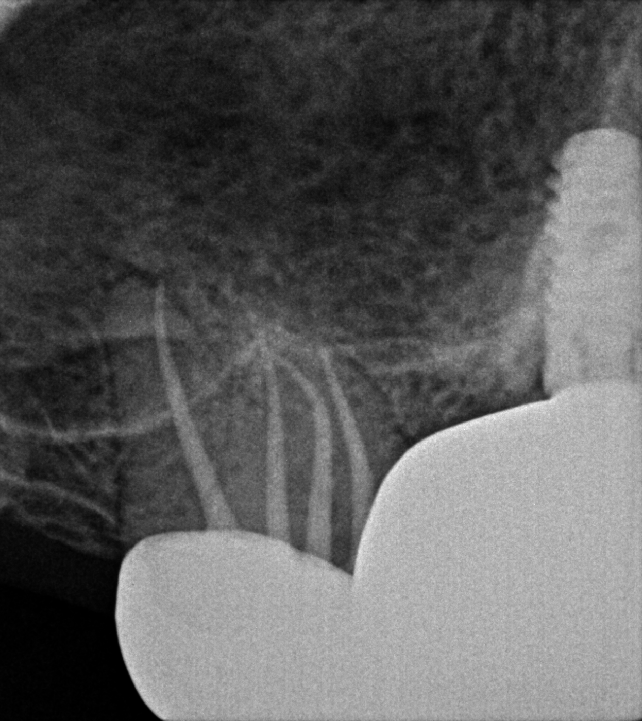
After completing a root canal it is important to get a final x-ray to verify that everything is sealed properly. Because every tooth is different, there is no set length for canals. Most dentists, myself included, use a tool called an apex locator to figure out how long the canal is. But it is important to always check your work with a final x-ray!


In most cases, when doing a root canal on a crown, unless the crown needs to be replaced, we just go straight through the crown to perform the root canal. When we finish, we put a filling in the hole and call it a day. I expect this tooth to give our patients many years of good use and millions of chews!