We recently documented a two-stage implant placement to share here on the blog. I previously shared one of my one-stage implant cases. If you don’t know the difference between a one-stage and a two-stage implant, refer back to that article because I cover it there in depth.
This two-stage case is one I inherited from a previous dentist at this practice. He had extracted the patient’s tooth and bone grafted almost one year ago. The patient was pregnant and wanted to have her baby before placing the implant. She delivered a healthy baby girl three weeks ago and was ready to get her implant started.
Planning
Remember that the first stage of a two-stage implant placement is tooth removal and bone replacement. Basically, we take out the tooth, then put bone graft in the socket. Once the bone has healed in three to six months, we can place an implant.
Just like the one-stage implant, the first step is always planning. The actual implant placement process is actually not all that difficult or complex. The hard part is planning the case properly.


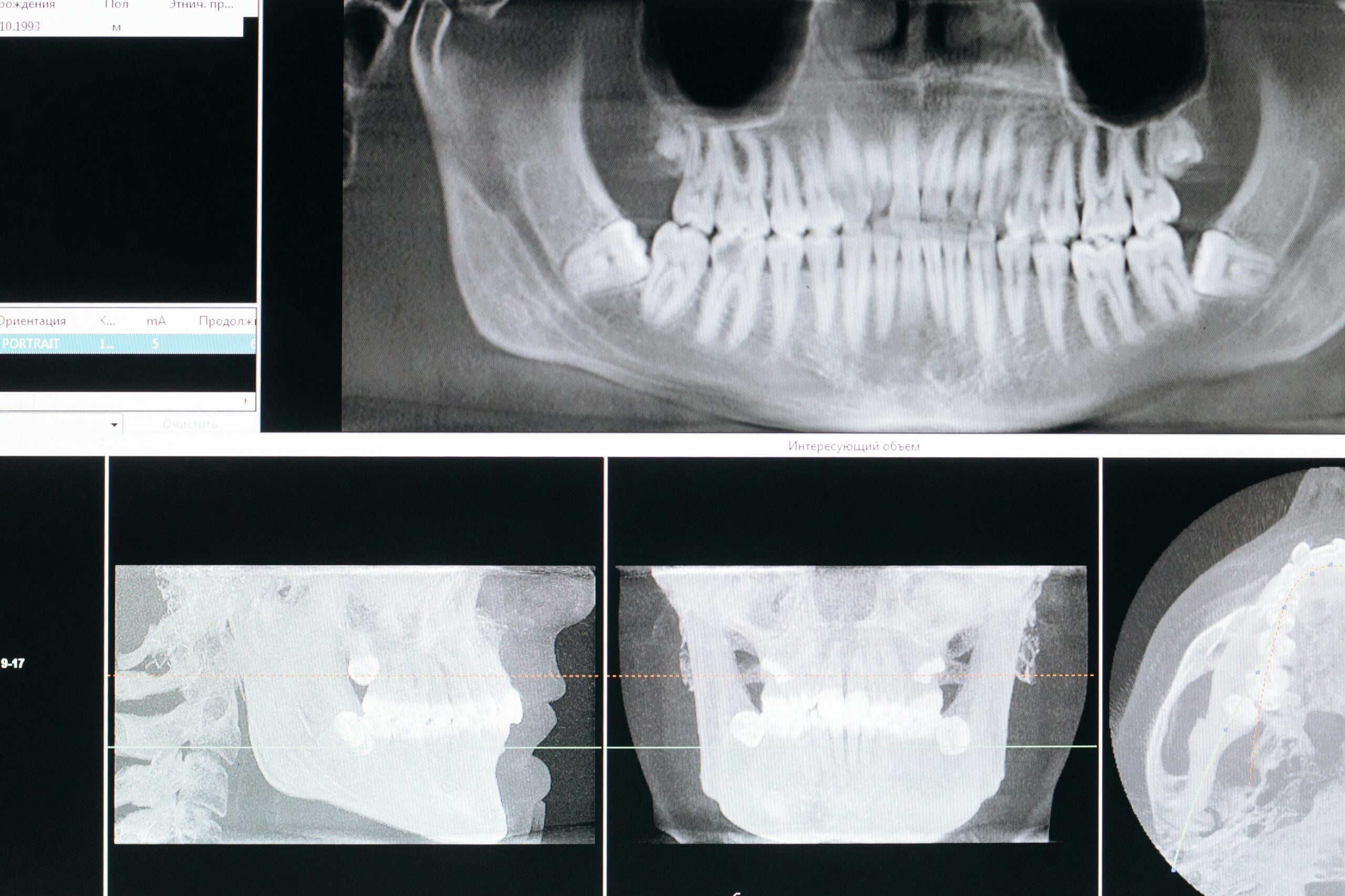
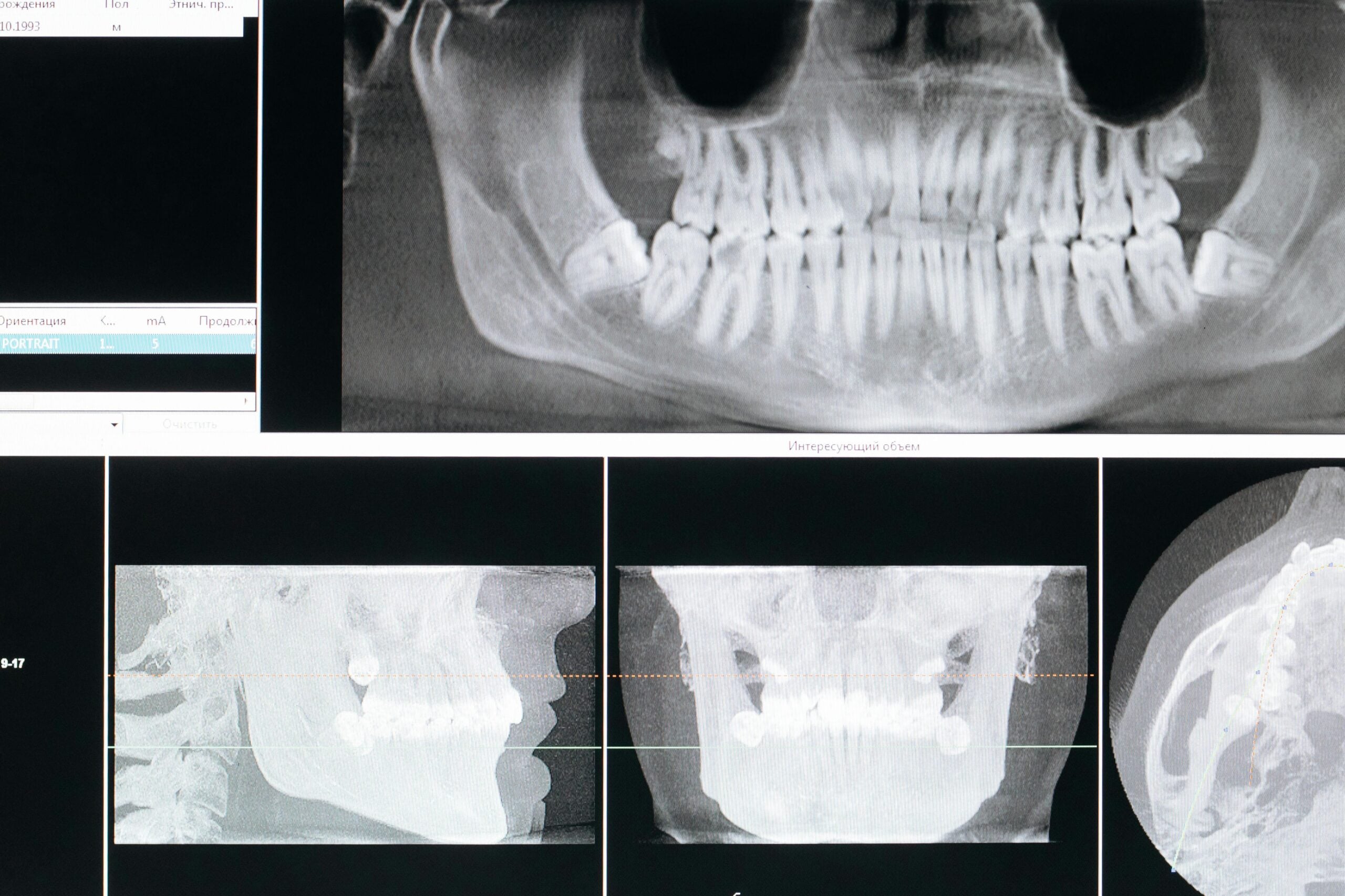
The above images come from a Cone Beam CT Scan, or CBCT for short. This x-ray gives us a 3-dimensional view of the area we will be working on. As you can see, we are looking at the implant from two different views.
There isn’t much room to work with here. The implant outline seen here is 3.5mm wide, which is the smallest diameter I have available in the office. The implant has plenty of room, but the implant crown is going to need to be fairly small. The screw that holds the crown to the implant will have to travel through the yellow rectangle. As you can see, that doesn’t leave much room on either side of the crown.
Preparation
Every dentist has different ways of preparing patients for implant surgery. I always have patients swish with 0.12% chlorhexidine mouth rinse for 30 seconds to reduce the microbial levels in their mouth. I also pre-medicate the patient with antibiotics.
We want to be sure the patient’s blood pressure is acceptable before we begin. We also want to be sure we have reviewed the patient’s health history and medication list. The patient must then read and sign all of the consent forms that are necessary to begin the procedure.
Finally, we discuss after-care instructions with the patient. We will discuss the same instructions again after the procedure. Reinforcing the instructions means it is more likely the patient will understand and remember them. In sedation cases, of course we want to be sure the patient is adequately sedated before we commence treatment.
We also want to make sure we have gone over all instructions with the patient before they are sedated. After the procedure, we will give instructions to the patient’s escort.
Implant Placement
After our patient is numb and comfortable, we will make an incision of the gum. Once we have opened the gum and exposed the underlying bone, I use a sharp drill to make a small hole where I want my hole to go. Then, I use my pilot drill and drill to the desired depth.

After the pilot drill, I place a guide pin to check my angles. Because teeth grow in all sorts of directions, it sometimes appears that you are drilling at the right angle but really you are way off course. This is why I always take an x-ray with a guide pin as shown below, apologies for the image quality.

Once we are sure that we are headed in the right direction, we widen the hole. I tell patients that placing an implant is like hanging a picture on the wall. First you find the stud, then you drill a small hole. The bigger the screw you want to place, the more drills you need to use to get there.

After seeing the amount of bone I had to work with and the restorative space, I decided to increase my implant size a bit. Remember that my original plan from the CBCT was to use a 3.5mm implant, but the space was able to accommodate a 3.75mm implant of the same length.
Closing Up
After the implant is placed, we have to decide if we are going to bury it under the gum, or put a healing abutment on top. The healing abutment allows the gum to heal so the crown will emerge from the gum like a natural tooth. If we can place the healing abutment the same day we place the implant, then we seat the crown 3-4 months sooner.


We achieved the maximum amount of torque for our implant, so I felt comfortable placing the healing abutment. As you can see from the above images, we successfully closed the gum around the healing abutment with two sutures.
Placing implants into tight spaces can be difficult, the tolerances are measured in millimeters or less. In the case of this implant we had about half a millimeter on each side we could work with. Below is an image showing how centered our implant is on the x-ray. The above images are taken at an angle, so the healing abutment looks off center.

Final Restoration
Our patient will return in around three months to take final impressions for her crown. This implant has an excellent chance of succeeding. Virtually every factor that contributes to the success of an implant was achieved in this case. We encountered no complications and the patient experienced no post-operative problems.
In a few months I will try to post images of the final crown.